NCLEX Infection Control: Decide by Route of Transmission
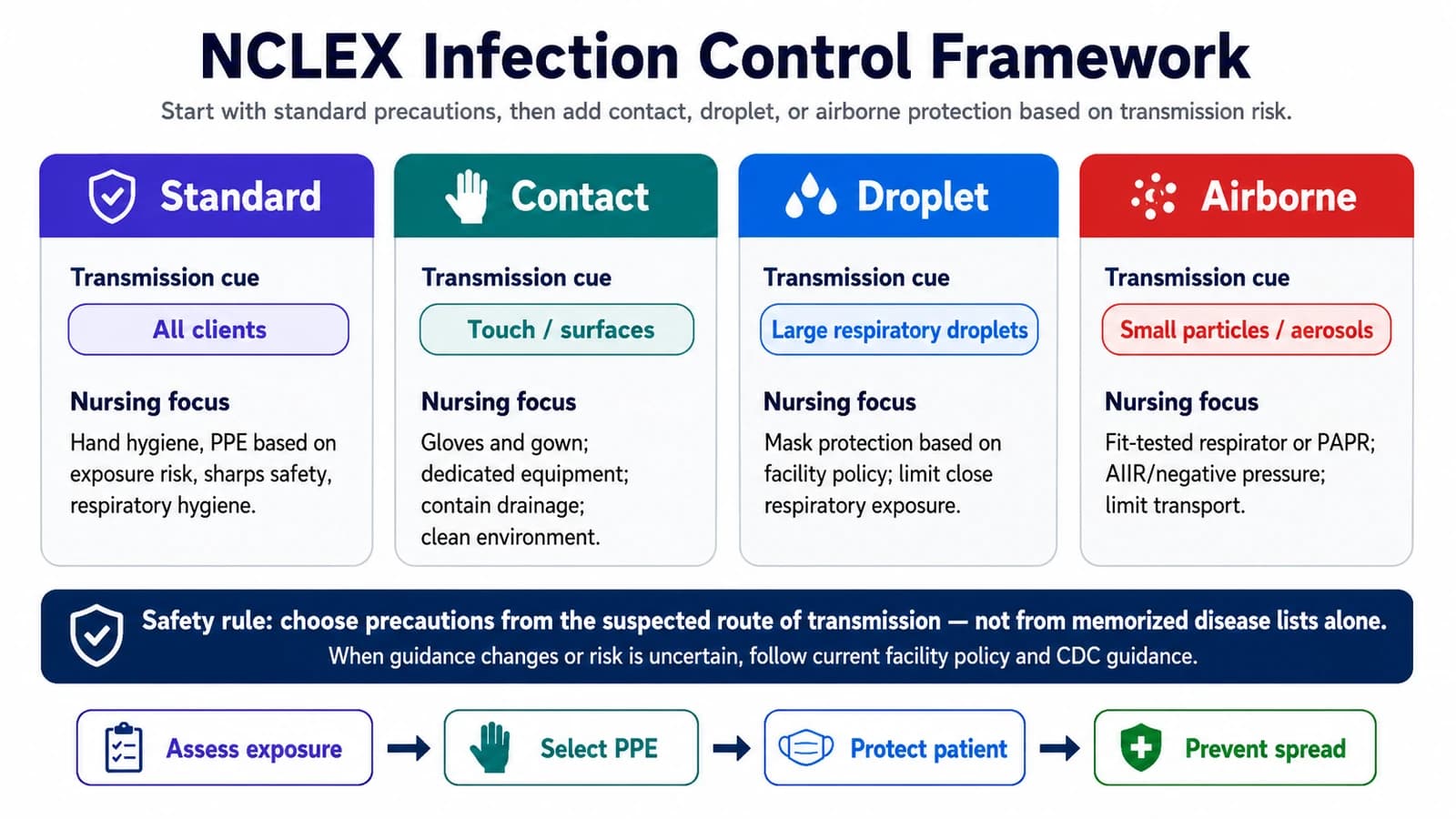
A reliable way to answer infection-control questions is to think about the route of transmission and the safest nursing action — not to memorize disease lists. Start with standard precautions, add the right barrier for the suspected route, and let current guidance fill in the details.
Infection control appears within the NCLEX Safety and Infection Prevention and Control content, which is about protecting clients and health care personnel from hazards. You do not need to memorize every organism. You need a reliable way to reason from the suspected route of transmission to the safest nursing action, guided by facility policy and current CDC recommendations.
Quick Answer: How to Think About Infection Control on the NCLEX
Use a route-and-safety approach rather than rote disease lists:
- Start with the suspected route of transmission — contact, droplet, or airborne — rather than memorizing disease lists.
- Apply standard precautions to every client, then add transmission-based precautions when a route is known or suspected.
- Let facility policy, isolation signage, and current CDC guidance decide the exact PPE, room, and transport details.
- For each scenario, ask what protects the client, what protects you and other staff, and what interrupts the chain of infection.
- Practice questions that ask which action is safest, then review the reasoning behind the answer.
To see how this fits the test plan and item formats, review the NCLEX Client Needs categories, the NCLEX question types guide, and the Next Generation NCLEX guide.
What NCLEX Infection Control Really Tests
Most items reward safe nursing judgment rather than trivia. Expect questions that ask you to:
- Match the right precautions to a suspected route of transmission
- Choose appropriate PPE for the anticipated exposure
- Recognize when hand hygiene calls for soap and water rather than alcohol-based rub
- Apply sterile technique and identify when a field is contaminated
- Respond safely to a sharps injury or body-fluid exposure
- Protect clients at higher infection risk, such as those who are neutropenic or have invasive devices
The Infection-Control Framework
When you meet any infection scenario, run it through the same steps. This habit generalizes far better than memorized disease lists.
Reason from the suspected route of transmission to the safest nursing action, guided by current policy.
Suspected route
Is transmission by contact, droplet, or airborne spread? The route drives the precautions, even before a diagnosis is confirmed.
Standard precautions first
Apply hand hygiene and standard precautions to every client, treating all blood and body fluids as potentially infectious.
Add the right barrier
Layer on transmission-based precautions and PPE matched to the anticipated exposure and the facility's isolation guidance.
Protect everyone
Consider the client, yourself, other staff, and other clients — source control, room placement, and equipment all matter.
Follow current guidance
Confirm the specifics against facility policy, isolation signage, and current CDC recommendations rather than a fixed memory rule.
Standard Precautions: The Baseline for Every Client
Standard precautions apply to the care of every client, regardless of suspected or confirmed infection status. They assume that blood, body fluids, non-intact skin, and mucous membranes may carry infectious agents. They include hand hygiene, PPE matched to the anticipated exposure, respiratory hygiene and cough etiquette, safe injection practices, and safe handling of potentially contaminated equipment and surfaces.
Hand Hygiene: When Alcohol Rub vs. Soap and Water Matters
Alcohol-based hand rub is preferred in many routine situations when hands are not visibly soiled. Soap and water is important when hands are visibly soiled and for spore-forming organisms such as C. difficile, where alcohol-based products are less effective against spores. Perform hand hygiene at these moments:
Key moments for hand hygiene
- Before and after contact with each client
- Before an aseptic or sterile procedure
- After contact with blood, body fluids, or contaminated surfaces
- After removing gloves
- When moving from a soiled to a clean site on the same client
PPE Selection: Anticipated Exposure, Not Memorized Habit
Choose PPE for what you expect to encounter, and follow your facility's sequence for putting it on and taking it off.
- Choose PPE based on the anticipated exposure, not habit — gloves for contact with body fluids, gown when clothing may be soiled, mask and eye protection when splashes or sprays are possible.
- Put PPE on and take it off in the sequence your facility specifies; the goal is to avoid contaminating yourself while removing it.
- Gloves typically come off first during removal because they are the most contaminated, followed by hand hygiene.
- Perform hand hygiene after removing PPE, and again whenever indicated.
Contact Precautions
Used when transmission is by direct or indirect contact with the client or their environment.
Traditional NCLEX teaching often groups examples such as multidrug-resistant organisms, C. difficile, scabies, and wounds with heavy drainage here. Always confirm precautions against current isolation guidance, since some organisms require added measures.
Droplet Precautions
Used when transmission is by respiratory droplets generated during coughing, talking, or certain procedures.
Examples traditionally taught here include influenza, pertussis, and meningococcal disease. The exact PPE and room details should follow current CDC guidance and facility policy rather than a single fixed rule.
Airborne Precautions
Used when transmission is by small airborne particles that can remain suspended and travel beyond the immediate area.
Conditions traditionally taught here include tuberculosis, measles, and varicella. Some pathogens require both airborne and contact precautions; follow current guidance for the specific situation.
Contact vs. Droplet vs. Airborne: A Comparison
This comparison summarizes the typical pattern. Treat it as a study aid — the exact PPE, room, and transport details for a given client follow current CDC guidance and facility policy.
| Feature | Contact | Droplet | Airborne |
|---|---|---|---|
| Primary route | Direct/indirect contact | Respiratory droplets at close range | Small airborne particles |
| Typical PPE | Gloves + gown | Mask per policy/pathogen | Fit-tested N95 or PAPR |
| Room | Private preferred | Private preferred | Negative-pressure room, door closed |
| Transport | Minimize; clean surfaces | Client mask as appropriate | Limit transport; client source control |
| Examples often taught | MDROs, C. difficile, scabies | Influenza, pertussis, meningococcal | Tuberculosis, measles, varicella |
Chain of Infection: Where Nurses Interrupt Transmission
Infection requires every link in the chain. Breaking any single link interrupts transmission, which is why understanding the chain helps you choose where to act.
| Link | What it is | How nurses interrupt it |
|---|---|---|
| Infectious agent | The pathogen | Cleaning, disinfection, sterilization, antimicrobial stewardship |
| Reservoir | Where it lives and multiplies | Environmental cleaning, wound care, food safety |
| Portal of exit | How it leaves the reservoir | Cover coughs, contain drainage, manage waste |
| Mode of transmission | How it travels | Hand hygiene, PPE, transmission-based precautions |
| Portal of entry | How it enters a new host | Aseptic technique, catheter and wound care |
| Susceptible host | Who is vulnerable | Vaccination, nutrition, protecting at-risk clients |
Medical Asepsis vs. Surgical Asepsis
Telling clean technique from sterile technique is a recurring NCLEX theme, because it changes what counts as a safe action.
Medical asepsis (clean technique)
- Reduces the number and spread of microorganisms
- Hand hygiene, clean gloves, environmental cleaning
- Used for routine care such as vital signs, bathing, and many bedside tasks
Surgical asepsis (sterile technique)
- Aims to maintain a sterile field and prevent the introduction of microorganisms
- Sterile gloves, sterile field, sterile supplies
- Used for procedures such as urinary catheter insertion, sterile dressing changes, and central line care
Sterile Field Rules
Sterile field management is a practical, clinically safe skill the NCLEX returns to often. Keep these principles in mind.
- Only sterile items touch a sterile field; if an unsterile item contacts it, treat the field as contaminated.
- Treat the outer edge of the sterile drape as a non-sterile border and keep items toward the center.
- Keep the sterile field in view and do not turn your back on it or reach across it.
- Keep the field dry, since moisture can carry microorganisms across the barrier.
- Hold sterile items above waist level and within your line of sight.
- Open sterile packages away from you so you do not reach over the field.
- When in doubt, consider the field contaminated and start over — that is the safe choice.
Practice NCLEX Infection-Control Questions
Work through adaptive NCLEX-style infection-control questions with rationales that explain the safest action and the route-of-transmission reasoning behind it.
Start PracticingSharps Safety and Exposure Response
Sharps injuries are a recognized occupational hazard, and the NCLEX tests both prevention and the response after an exposure.
- Activate safety features on devices and avoid recapping needles.
- Dispose of sharps at the point of use in a puncture-resistant container, and do not overfill it.
- Use safer-engineered devices and work practices supported by your facility's sharps-safety program.
- After an exposure: wash the site, report it promptly, and follow facility protocol for evaluation and any indicated prophylaxis.
Special Infection-Risk Situations
Some clients face higher infection risk and need added vigilance. These patterns appear regularly in NCLEX scenarios.
Neutropenia
Clients with very low neutrophil counts need protective measures per policy; fever may be the only early sign of infection, so monitor closely and minimize exposure to potential sources.
Central lines
Follow the central-line care bundle — hand hygiene, aseptic technique, appropriate site care, and daily review of whether the line is still needed — to reduce bloodstream-infection risk.
Urinary catheters
Maintain a closed drainage system, keep the bag below bladder level, provide routine care, and remove the catheter as soon as it is no longer needed.
Post-op wounds
Assess incisions for signs of infection, use aseptic technique for dressing changes, and teach clients what to report after discharge.
Older adults
Infection can present atypically and without fever; a change in mental status, appetite, or function may be the earliest clue.
Many of these decisions draw on the same reasoning as the NCLEX clinical judgment framework, and several connect to medication safety covered in our pharmacology basics guide.
What to Do When Precautions Are Unclear
When you are unsure which precautions apply, default to the safer choice and confirm — never guess and proceed.
The safe sequence
- Default to standard precautions for every client, always.
- When the route is uncertain, choose the more protective precautions until it is clarified.
- Check the isolation signage and the medical record, and confirm with the charge nurse or infection preventionist.
- Follow facility policy, current CDC guidance, provider orders, and your nursing scope of practice.
- Document the precautions in place and any clarification you obtained.
A Study Plan for Infection-Control Questions
A sustainable plan builds route-based reasoning first, then layers in nursing actions and practice.
Anchor on routes
Learn the three transmission routes and the barrier each one calls for before drilling individual diseases.
Layer in nursing actions
For each route, attach hand hygiene, PPE, room placement, and transport principles — framed as 'follow current guidance,' not fixed rules.
Practice in context
Use questions and NGN case studies that ask which action is safest, then review every rationale.
Target your misses
Keep a short list of the scenarios you get wrong and revisit them rather than re-reading what you already know.
Fit this into a realistic timeline with the 30/60/90 NCLEX study plan and our NCLEX study tips.
Build Your NCLEX Study Plan
Turn this approach into a weekly schedule with adaptive practice, NGN-style questions, rationales, and performance feedback. Use the feedback to decide what to review next.
Build Your Study PlanSources and Alignment Note
How this guide was reviewed
Reviewed against current NCLEX Safety and Infection Prevention and Control content and CDC infection-control guidance. This page is educational NCLEX preparation content and does not replace facility policy, isolation signage, current CDC guidance, provider orders, or clinical judgment. RN Test Pro is independent and not affiliated with or endorsed by NCSBN. NCLEX® is a registered trademark of the National Council of State Boards of Nursing, Inc.
Related Resources
Infection Control: Full Safety & Infection Control Guide →
The broader Safety and Infection Control category overview and reference.
Pharmacology Basics →
Study medications as safety and clinical judgment, not memorization.
Clinical Judgment →
The recognize–analyze–act–evaluate model behind safe decisions.
Next Generation NCLEX →
How case studies test infection-control judgment across steps.
30/60/90 Study Plan →
Fit infection control into a realistic timeline you can sustain.
RN NCLEX Prep →
Adaptive practice built for the RN candidate path.
PN NCLEX Prep →
Adaptive practice built for the PN candidate path.