NCLEX Pharmacology Basics: How to Study Medications Safely
Pharmacology feels overwhelming when you try to memorize every drug. The NCLEX is really testing safety and clinical judgment — so the fastest way to improve is to learn medication classes, the assessments and labs that matter, and when to question an order.
Pharmacology appears across NCLEX Client Needs categories and shows up in many safety decisions. You do not need to memorize every drug. You need to know common medication classes and safety patterns well enough to reason through an unfamiliar drug, recognize danger, and choose the safest action.
For the full exam-aligned study framework, see our NCLEX pharmacology guide; this article focuses on the practical bedside skills — the rights of medication administration, telling expected effects from adverse ones, and what to do when an order looks unsafe.
Quick Answer: How to Study Pharmacology for the NCLEX
Use a class-and-safety approach rather than brute-force memorization:
- Learn medication classes and their shared patterns instead of memorizing every individual drug.
- For each class, focus on what it does, the main adverse effects, the assessments and labs that matter, and the contraindications.
- Practice questions that ask what to assess, what to teach, and when to clarify an order — not just what a drug is for.
- Tie each medication to safety: airway, circulation, bleeding, electrolytes, and level of consciousness.
- Review rationales so you understand why an answer is the safest action, then keep a short list of the patterns you miss.
To organize this into a timeline, see the 30/60/90 NCLEX study plan, and pair it with our NCLEX study tips for active recall and rationale review.
What NCLEX Pharmacology Really Tests
Most pharmacology items are about safe nursing action, not trivia. Expect questions that ask you to:
- Recognizing a class from its suffix or prototype and predicting its effects
- Choosing the right assessment or lab before and after administration
- Identifying adverse effects that require holding the dose and clarifying with the provider
- Spotting contraindications, interactions, and unsafe orders
- Teaching clients what to expect, what to report, and how to take a medication safely
- Applying clinical judgment in NGN case studies that unfold over several steps
For how these map to the test plan and item formats, see the NCLEX Client Needs categories, the NCLEX question types guide, and the Next Generation NCLEX guide.
The Pharmacology Safety Framework
When you meet any medication — even one you have never seen — run it through the same five steps. This is the habit the NCLEX rewards.
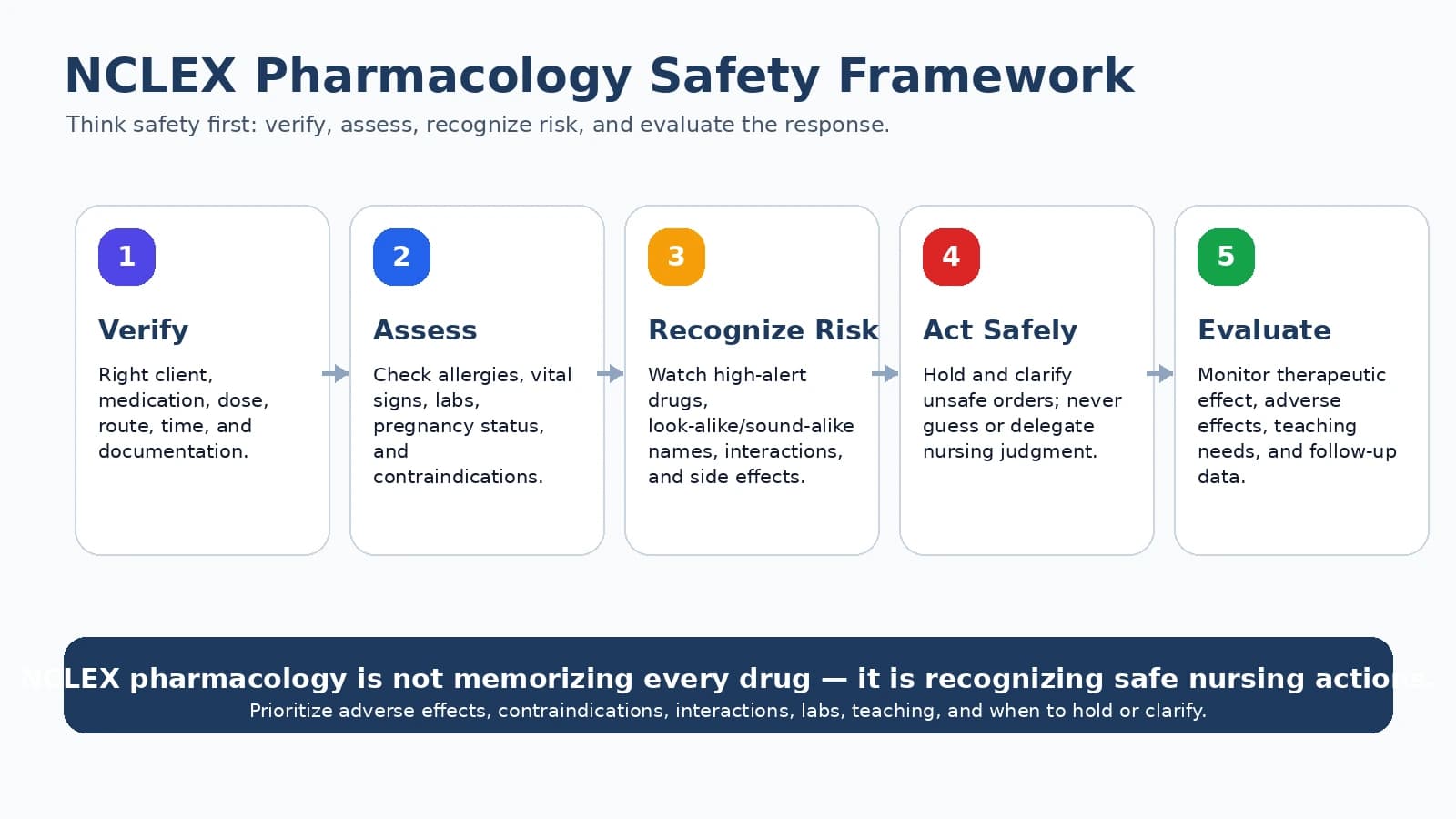
Run every medication through the same safety steps, from class and assessment to teaching and evaluation.
Class & purpose
What family is this drug in, and what is it being used to treat for this client?
Assess first
What vital signs, labs, allergies, and baseline findings should you check before giving it?
Adverse effects
What serious reactions would make you hold the dose and clarify with the provider?
Contraindications & interactions
Does the client's history, pregnancy status, other medications, or diet make this unsafe?
Teach & evaluate
What does the client need to know, and how will you judge whether the medication is working safely?
Medication Administration Rights: A Safety Checklist, Not a Shortcut
The “rights” are a safety checklist, not a box-ticking ritual. They appear constantly on the NCLEX, and the exam often tests them by giving you a situation where one right is violated. The traditional five have expanded in modern practice to include several more.
| Right | What it means in safe practice |
|---|---|
| Right client | Use two identifiers (such as name and date of birth or MRN). A room number alone is not an identifier. |
| Right medication | Verify against the order and the medication record; check allergies and interactions. |
| Right dose | Verify the calculation, especially weight-based and pediatric doses; question doses that fall outside a safe range. |
| Right route | Confirm the ordered route; never assume. Some drugs are dangerous by the wrong route. |
| Right time | Give within the window allowed by facility policy for that medication; time-critical drugs are stricter. |
| Right documentation | Document after giving the medication, never before. |
| Right reason | Confirm the indication matches the client; if the drug does not fit the diagnosis, clarify. |
| Right response | Evaluate effectiveness and watch for adverse effects after giving it. |
| Right to refuse | A competent client may refuse; document and notify the provider as appropriate. |
| Right education | Teach the purpose, what to report, and how to take it safely. |
Note the “right time” is governed by facility policy for each medication rather than a single universal number; time-critical medications have tighter windows. When any right cannot be satisfied, the safe action is to stop and clarify.
What to Know for Each Medication Class
For each class, anchor on four things: what it does, the adverse effects that matter, the assessments and labs that go with it, and the contraindications. The table below shows the safety pattern for several common classes — learn the pattern, and individual drugs become easier to reason about.
| Class | What it does | Safety pattern to know |
|---|---|---|
| ACE inhibitors (-pril) | Lower blood pressure; reduce cardiac workload | Dry cough, elevated potassium, first-dose hypotension, angioedema (airway emergency); avoid in pregnancy |
| Beta blockers (-olol) | Lower heart rate and blood pressure | Assess heart rate before giving; can blunt the warning signs of low blood sugar; caution with reactive airway disease; do not stop abruptly |
| Anticoagulants | Reduce clot formation | Bleeding is the key risk; know the relevant monitoring test and reversal agent for each, and assess for signs of bleeding |
| Diuretics | Remove excess fluid | Track electrolytes (especially potassium) and fluid status; loop and thiazide agents tend to lower potassium, while potassium-sparing agents can raise it |
| Opioids | Relieve moderate to severe pain | Watch sedation and respiratory rate; keep the reversal agent available; anticipate constipation |
| Insulin | Lower blood glucose | Match type to onset/peak; confirm dose carefully; monitor glucose and watch for hypoglycemia |
| Antibiotics | Treat infection | Assess allergies before every dose; obtain cultures before the first dose when ordered; watch for superinfection |
These are study-level patterns, not administration instructions. Always confirm specifics against a current medication reference, the provider order, and facility policy.
High-Risk Medication Patterns the NCLEX Emphasizes
Rather than memorizing endless detail, recognize the recurring high-risk patterns. Most dangerous-medication questions fall into one of these.
Narrow therapeutic range
Drugs such as digoxin and lithium have a small gap between a helpful and a harmful level. NCLEX focuses on assessment, recognizing toxicity, and knowing when a level should be checked — not on memorizing exact numbers.
Bleeding risk
Anticoagulants and antiplatelets center on bleeding precautions, the right monitoring test, the reversal agent, and teaching clients what bleeding to report.
Electrolyte shifts
Diuretics, potassium, and some cardiac drugs interact through potassium and other electrolytes. Concentrated IV potassium is never given by IV push.
Respiratory or sedation risk
Opioids, sedatives, and some anesthetics share the pattern of monitoring sedation and breathing and keeping a reversal agent ready.
High-alert double-checks
Insulin, heparin, chemotherapy, and concentrated electrolytes are commonly verified with an independent second nurse per facility policy.
For digoxin, lithium, vancomycin, anticoagulants, insulin, opioids, potassium, and antihypertensives, the NCLEX rewards the same instincts: assess the client, check the relevant labs, recognize adverse effects and contraindications, and clarify the order when something does not fit. Exact therapeutic ranges are best confirmed against a current reference rather than memorized as trivia.
Labs and Vital Signs Before Giving Medications
Many NCLEX items hinge on a single assessment or lab you should check before administering. The skill is matching the right check to the drug, then deciding whether the finding makes the dose safe to give.
| Medication group | Check before / after | How it guides the safe action |
|---|---|---|
| Antihypertensives & antiarrhythmics | Blood pressure and heart rate | Reassess the parameter the drug affects; clarify when readings fall outside the ordered limits for that client |
| Anticoagulants | The relevant clotting study for that drug | Assess for bleeding; results outside the target range are a reason to clarify before giving |
| Digoxin | Heart rate and potassium | Recognize toxicity (such as visual changes, nausea, rhythm changes); a level may be ordered if toxicity is suspected |
| Diuretics | Potassium and fluid status | Low or high potassium can change whether the dose is safe to give |
| Insulin | Blood glucose | Confirm glucose and the client's intake; treat hypoglycemia before it worsens |
| Nephrotoxic or hepatotoxic drugs | Kidney or liver studies | Trends matter; rising values may mean the dose needs review |
Build the underlying number sense with our guide to lab values every nursing student should know.
Adverse Effects vs. Side Effects vs. Expected Effects
NCLEX questions often turn on telling these three apart, because the category determines your action.
Expected (therapeutic) effect
The intended result — a beta blocker lowering an elevated heart rate, or an analgesic reducing pain. You evaluate for this to judge effectiveness.
Side effect
A predictable, usually tolerable effect that is not the goal — such as mild drowsiness. Often managed with teaching and monitoring.
Adverse effect
A harmful, often serious reaction — such as angioedema, severe bleeding, or respiratory depression. This is the category that prompts you to hold the dose and clarify with the provider.
A reliable test-taking instinct: an expected finding usually means continue and monitor, a side effect usually means teach and monitor, and an adverse effect usually means hold the dose and clarify with the provider.
Drug Interactions and Contraindications
Most interaction questions fit a few recognizable types:
- Drug–drug: combinations that amplify a shared effect (for example, several agents that all increase bleeding risk or all lower blood pressure).
- Drug–food: foods that change a drug's effect (for example, large swings in vitamin K intake with warfarin).
- Drug–condition: a client's history, organ function, or pregnancy status that makes a drug unsafe.
- Allergies: always reconcile allergies before administration, and treat a documented serious reaction as a contraindication.
When a client's history or current medications make a drug unsafe, treat that as a reason to clarify before giving — not a detail to work around.
Client Teaching Patterns
Teaching items reward clear, safety-focused communication. Most correct answers cover some combination of:
- What the medication is for, in plain language
- How and when to take it, and what to do about a missed dose
- Which adverse effects to report right away
- Foods, drinks, or other medicines to avoid
- Not to stop certain medications abruptly without provider guidance
- How to store it and keep it away from children
Practice NCLEX Pharmacology Questions
Work through adaptive NCLEX-style pharmacology questions with rationales that explain the safest action and the assessment behind it. Use the feedback to target your weak patterns.
Start PracticingWhat to Do When an Order Looks Unsafe
One of the most important pharmacology instincts the NCLEX tests is refusing to give a medication that appears unsafe. Ordered does not mean safe.
The safe sequence
- Do not give a medication you believe is unsafe just because it was ordered.
- Check the order against the medication record, the client's allergies, and a current drug reference.
- Verify the dose, route, and frequency, and confirm the indication fits the client.
- Hold and clarify with the prescriber when assessment data, labs, or the order itself suggest risk.
- Follow facility policy, the medication reference, the provider order, and your nursing scope of practice.
- Medication judgment stays with the licensed nurse and is not delegated to unlicensed assistive personnel.
- Document your assessment, the concern, and the provider's response.
The same judgment underlies the NCLEX clinical judgment framework: recognize the cue, decide what it means, act safely, and evaluate.
A Pharmacology Study Plan
A sustainable plan builds class knowledge first, then layers safety and practice on top.
Build class scaffolding first
Spend early sessions learning the major classes by purpose, prototype, and shared adverse-effect pattern.
Layer in safety
For each class, attach the key assessments, labs, contraindications, and the situations that call for clarifying an order.
Practice in context
Use questions and NGN case studies that ask what to assess, teach, or clarify — then review every rationale.
Target your misses
Keep a short running list of the patterns you get wrong and revisit them, rather than re-reading content you already know.
Build Your NCLEX Study Plan
Turn this approach into a weekly schedule with adaptive practice, NGN-style questions, rationales, and performance feedback. Use the feedback to decide what to review next.
Build Your Study PlanSources and Alignment Note
How this guide was reviewed
Reviewed against current NCLEX test-plan pharmacology categories and medication-safety principles. This page is educational NCLEX preparation content and does not replace facility policy, medication references, provider orders, or clinical judgment. RN Test Pro is independent and not affiliated with or endorsed by NCSBN. NCLEX® is a registered trademark of the National Council of State Boards of Nursing, Inc.
Related Resources
Lab Values for NCLEX →
Reference ranges and the nursing actions that follow abnormal results.
Clinical Judgment →
The recognize–analyze–act–evaluate model behind safe medication decisions.
Next Generation NCLEX →
How case studies test medication safety across several steps.
30/60/90 Study Plan →
Fit pharmacology into a realistic timeline you can sustain.
RN NCLEX Prep →
Adaptive practice built for the RN candidate path.
PN NCLEX Prep →
Adaptive practice built for the PN candidate path.