NCLEX Fundamentals Guide: What This Topic Includes on the Exam
"Fundamentals" is a study label, not an official NCLEX category. On the NCLEX-RN, fundamentals content appears across Client Needs categories and integrated processes such as the nursing process, clinical judgment, communication and documentation, teaching and learning, and basic patient-care decisions.
Built around the current NCLEX-RN test plan and current infection-control guidance.
Where Fundamentals Shows Up on the NCLEX
The NCLEX does not have a "Fundamentals" category. Instead, fundamentals content is distributed across Client Needs categories and integrated processes.
| Fundamentals Study Area | Where It Appears on the NCLEX |
|---|---|
| Nursing process and clinical judgment | Integrated processes across categories |
| Safety and infection control | Safety and Infection Prevention and Control |
| Basic hygiene, mobility, elimination, comfort | Basic Care and Comfort |
| Vital-sign changes, focused assessment, complications | Reduction of Risk Potential |
| Growth, development, prevention, health teaching | Health Promotion and Maintenance |
| Documentation, communication, teaching | Integrated processes across categories |
Nursing Process and Clinical Judgment
The nursing process remains a core framework for NCLEX thinking. The current RN test plan describes it as assessment, analysis, planning, implementation, and evaluation. The NCJMM does not replace the nursing process; it adds a structured way to measure clinical judgment in unfolding situations.
- Assessment: Collect and validate subjective and objective data.
- Analysis: Connect the findings and identify the priority problem or concern.
- Planning: Identify the intended outcome and safest goals.
- Implementation: Choose and carry out the safest nursing action.
- Evaluation: Compare outcomes with expectations and reassess as needed.
Clinical judgment on the NCLEX includes recognizing cues, analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes. Good fundamentals study should train this reasoning, not just memorization.
Assessment Basics and Red Flags
Fundamentals questions often test whether you can recognize deterioration early, perform a focused assessment, and respond to changes before a complication becomes severe.
Assessment Red Flags
- Worsening oxygenation or shortness of breath
- Falling blood pressure or weak perfusion
- Persistent tachycardia or tachypnea
- New confusion or disorientation
- Fever or hypothermia in the right context
- New pain, weakness, or neurologic change
NCLEX-Style Clinical Scenarios
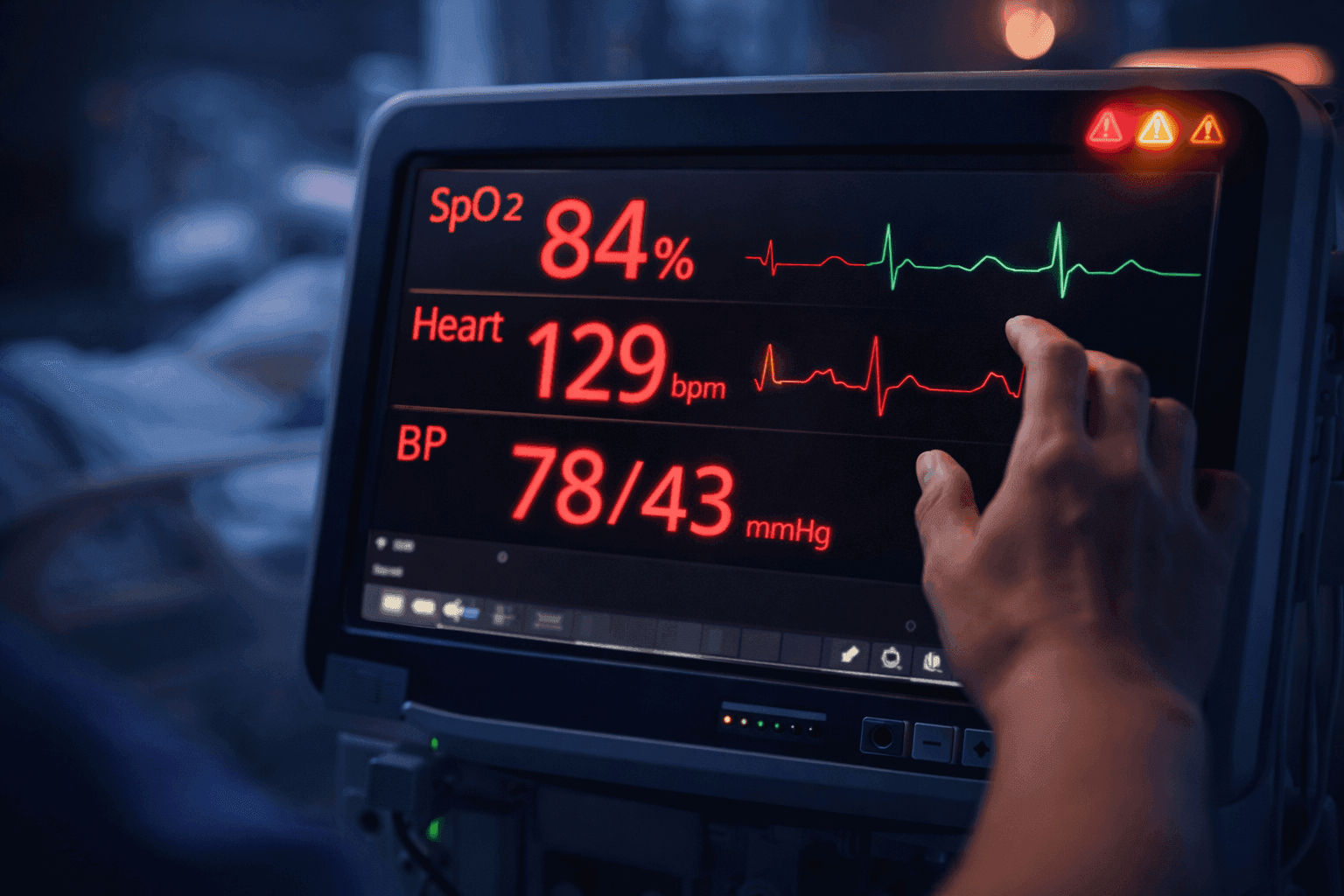
Vital Signs: Recognizing Acute Deterioration
A nurse is assessing a 68-year-old patient admitted with pneumonia. Vital signs: Temperature 102.2°F, HR 112 bpm, RR 28/min, BP 98/58 mmHg, SpO₂ 91% on room air. Which findings require immediate intervention?
Answer: All of these findings are concerning because they suggest acute deterioration: fever, tachycardia, tachypnea, borderline hypotension, and low oxygen saturation. The nurse should promptly reassess the patient, compare these findings with baseline status, support oxygenation per orders or protocol, and escalate quickly to the provider or team according to facility policy.
NCLEX Point: Recognize patterns of instability, not just isolated abnormal numbers. Fever, worsening oxygenation, tachypnea, poor perfusion, and mental-status changes should raise concern for serious infection, sepsis, or other acute deterioration and trigger urgent reassessment and escalation.
Focused Neurological Assessment
A nurse is performing a neurological assessment on a patient who had a stroke 3 days ago. The patient is alert but confused. Which components should the nurse include?
Answer: Level of consciousness, pupillary response (size, equality, reactivity), motor function (strength and movement in all extremities), sensory function, speech and swallowing, and changes from baseline. Document findings and report any deterioration.
NCLEX Point: Always compare with baseline. Any new deficit is urgent. Acute confusion is never a throwaway finding.
Head-to-Toe: Prioritizing Findings
A nurse documents: diminished breath sounds in the left base, 2+ peripheral edema bilaterally, capillary refill of 4 seconds, and confusion about time and place. Which finding is most concerning?
Answer: The most urgent concern is the cluster of possible perfusion and oxygenation problems, especially the new confusion combined with delayed capillary refill and abnormal cardiopulmonary findings. The nurse should reassess airway, breathing, circulation, oxygenation, neurologic status, and escalate based on the overall pattern of instability.
NCLEX Point: Do not isolate one abnormal finding without looking at the whole pattern. Prioritization depends on overall instability, especially changes in oxygenation, perfusion, and mental status.
Safety and Infection Control Essentials
Safety and infection-control questions test whether you can apply precautions correctly, prevent avoidable harm, and stop unsafe care before it reaches the patient.
Standard Precautions apply to all patient care. Transmission-Based Precautions are added when the patient may have an infection that requires extra measures to prevent spread.
| Precaution Type | Core Use |
|---|---|
| Standard Precautions | Used for all patient care |
| Contact Precautions | Added for contact transmission risk |
| Droplet Precautions | Added for droplet spread |
| Airborne Precautions | Added for airborne spread |
- Hand hygiene and PPE based on exposure risk
- Sterile field contamination means stop and correct
- Medication safety and SBAR communication are fundamentals-level safety skills
For deeper coverage, see our Safety and Infection Prevention and Control page.
Basic Care and Comfort Essentials
Basic care and comfort is not a low-value topic. It tests whether you can protect dignity, support daily function, and notice when basic care needs become safety problems.
Think beyond the task: If a patient is immobile and incontinent, think beyond hygiene. This affects skin integrity, comfort, dignity, infection risk, and repositioning needs.
Legal, Ethical, Communication, and Documentation Basics
- Informed consent and the nurse's role
- Patient rights and confidentiality
- Professional boundaries
- Clear communication with the team
- Accurate and timely documentation
- Patient teaching adjusted to readiness, barriers, and learning needs
The NCLEX does not separate safe care from communication and documentation. Poor handoff, weak documentation, and inadequate teaching can all turn a technically correct action into unsafe care.
How to Study Fundamentals for NCLEX
- Learn the official framework first — know how Client Needs categories and integrated processes organize the exam.
- Study red flags and focused assessments — these appear across many question types.
- Practice safety scenarios, not just fact lists — apply precautions and prioritization to realistic situations.
- Use case-based questions for fundamentals — connect assessment, intervention, and evaluation in each scenario.
- Review rationales for why the safest action is correct — this trains clinical judgment, not memorization.
When you are ready to organize your preparation, build a structured study plan.
Official Source
This page is built around the 2026 NCLEX-RN Test Plan (PDF) published by the National Council of State Boards of Nursing. It is for education and NCLEX preparation only and does not replace facility policy, instructor guidance, or employer procedures.
Practice Fundamentals Questions
Build your fundamentals base with focused practice on assessment, safety, basic care, and clinical judgment.
Practice Fundamentals QuestionsFrequently Asked Questions
What is the nursing process and how is it tested on NCLEX?
The nursing process includes assessment, analysis, planning, implementation, and evaluation. NCLEX tests your ability to apply this process in clinical scenarios. Assessment questions ask what data to collect, analysis questions ask about the priority problem, planning questions focus on goals and outcomes, implementation questions test nursing actions, and evaluation questions assess whether interventions were effective. These steps map directly to the CJMM: assessment aligns with recognizing cues, analysis with analyzing cues and prioritizing hypotheses, planning with generating solutions, implementation with taking action, and evaluation with evaluating outcomes.
What are the most important vital sign changes to recognize?
Look for changes in context: worsening oxygenation, tachypnea, falling blood pressure, persistent tachycardia, fever or hypothermia, weak perfusion, and any new confusion or disorientation. Trends and associated symptoms matter as much as the single number.
How often should I reassess my patient?
Reassess based on patient acuity, recent interventions, provider orders, changes in condition, and facility policy. Always reassess after significant interventions and with any new symptom or deterioration.
Is fundamentals an official NCLEX category?
No. Fundamentals is a study label used by nursing programs and prep resources. On the NCLEX, fundamentals content appears across Client Needs categories and integrated processes such as the nursing process, clinical judgment, communication and documentation, and teaching and learning.
Related NCLEX Topics
Clinical Judgment
The CJMM framework for NCLEX
Read moreSafety & Infection Control
Precautions, PPE, and patient safety
Read moreInfection Control
Transmission-based precautions in depth
Read moreDelegation
Five Rights and RN accountability
Read morePriority Questions
ABCs, Maslow, and acute vs chronic
Read morePharmacology
Medication safety and drug classes
Read moreCBC Guide
Lab values and clinical significance
Read moreBuild Your Personalized Study Plan
Create a tailored study plan based on your strengths and weaknesses. Track your progress and stay on schedule for exam day.
Create Study Plan