IV Therapy for NCLEX: Fluids, Complications, Calculations, and Safety
IV therapy questions test whether you can choose safe fluids, monitor IV sites, recognize complications, calculate rates, prevent infection, and respond quickly when an infusion harms the patient.
This topic is not just memorizing fluid names. NCLEX often asks:
- Which IV fluid is safest for this condition?
- Which IV site finding is most concerning?
- Is this infiltration, extravasation, phlebitis, infection, or fluid overload?
- What should the nurse do first?
- Which medication or fluid requires compatibility verification?
- What flow rate should the infusion pump be set to?
- What finding suggests a transfusion reaction?
- What response shows the intervention worked?
The safest strategy is to connect the IV therapy to the patient’s condition, the site assessment, the fluid or medication risk, and the expected response.
IV Therapy at a Glance
IV therapy appears mainly under Pharmacological and Parenteral Therapies, but it also overlaps with Reduction of Risk Potential and Physiological Adaptation. NCLEX may test:
- IV fluid types and tonicity
- Peripheral IV site assessment
- Infiltration, extravasation, phlebitis, infection, fluid overload, and air embolism
- Infusion-pump monitoring and IV flow-rate calculations
- Medication compatibility and high-risk IV medications
- Blood product administration and reaction response
- Central lines, PICCs, and TPN
- Patient response to parenteral therapy
- NGN case studies with changing vital signs, site findings, labs, and infusion orders
Scope reminder
About this guide
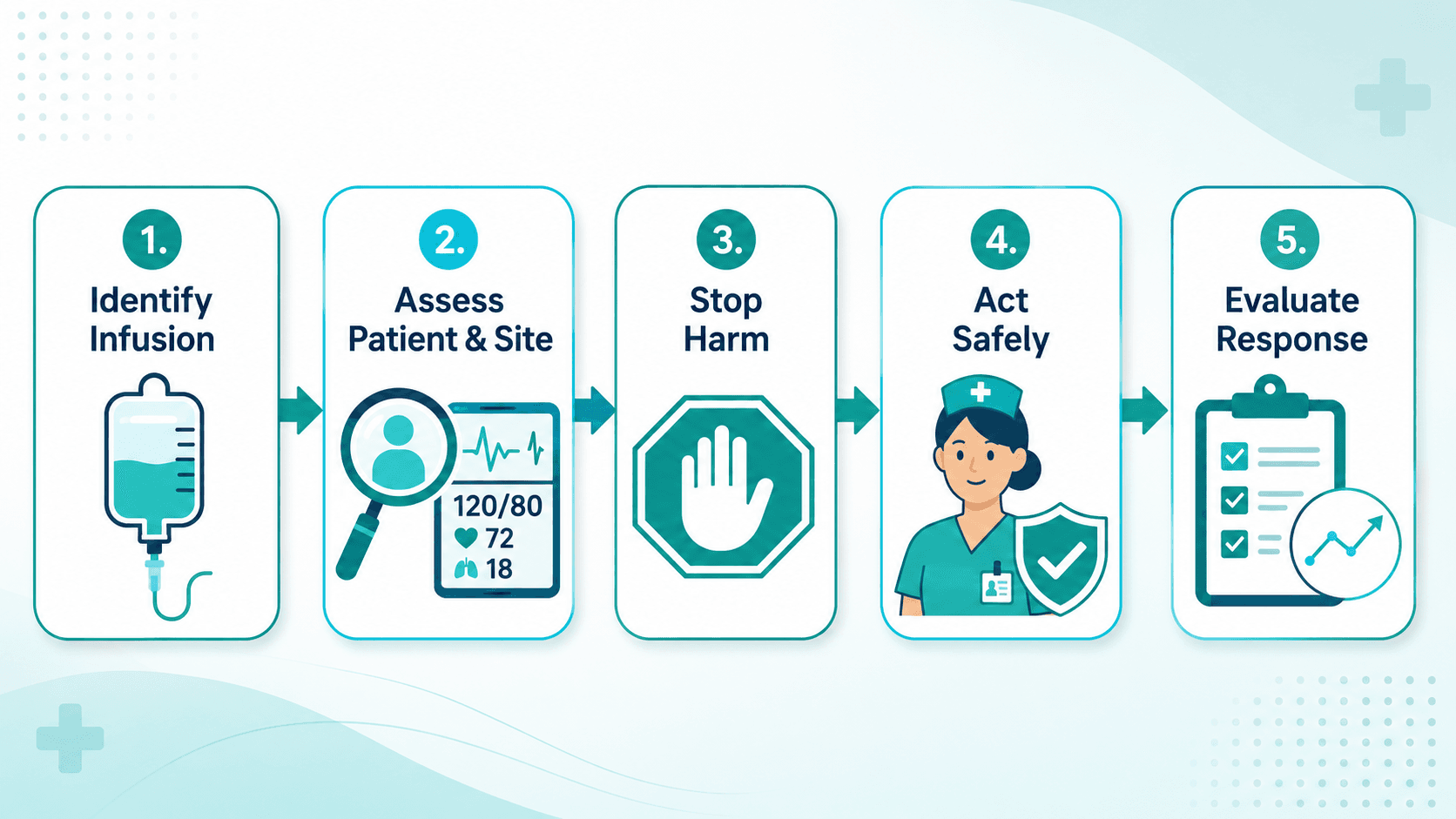
The IV Safety Framework
Use this five-step method for IV therapy questions.
1. Identify what is running
Is this isotonic, hypotonic, or hypertonic fluid? Is it a vesicant, irritant, blood product, electrolyte, TPN, antibiotic, insulin, heparin, or vasoactive medication? Is it compatible with the fluid and other medications? Does the patient have heart failure, kidney disease, increased ICP, dehydration, sepsis, or electrolyte imbalance?
2. Assess the patient and the site
Check the patient first when there are systemic symptoms: respiratory status, lung sounds, oxygen saturation, heart rate and blood pressure, mental status, and pain/burning. Then assess the IV site for color, temperature, swelling, drainage, and tenderness, plus the flow rate, pump alarms, and intake/output when fluid balance matters.
3. Stop the source of harm
If the IV site or infusion is causing harm, stop the infusion or stop using the line per policy. For example: infiltration → stop and remove the peripheral catheter unless policy says otherwise; extravasation → stop, disconnect tubing, leave the catheter initially for aspiration/antidote; fluid overload → stop/slow as ordered while supporting breathing; air in tubing → clamp before air enters the patient; suspected transfusion reaction → stop the transfusion immediately.
4. Act safely within scope
Safe actions may include raising the head of the bed, applying oxygen per order/protocol, clamping/stopping the infusion, removing or preserving the catheter depending on the complication, elevating the extremity, applying a warm or cold compress based on policy and infusate, notifying RN/provider/pharmacy/blood bank, starting a new IV if continued access is needed and allowed, monitoring vital signs and symptoms, and documenting objective findings.
5. Evaluate response
Ask whether swelling stopped increasing, pain improved, breathing/oxygenation improved, vital signs stabilized, the infusion rate matched the order, labs trended as expected, and whether the patient developed a reaction or complication.
IV Fluid Types for NCLEX
| Fluid type | Examples | Main effect | Common NCLEX use | Major danger |
|---|---|---|---|---|
| Isotonic | 0.9% sodium chloride, Lactated Ringer's | Expands extracellular/intravascular volume | Fluid resuscitation, dehydration, shock, blood-product line with normal saline | Fluid overload, especially with heart failure or kidney disease |
| Hypotonic | 0.45% sodium chloride; D5W after the dextrose is metabolized | Moves water into cells | Hypernatremia or cellular dehydration when ordered | Cerebral edema, worsening increased ICP, hypotension |
| Hypertonic | 3% sodium chloride; some dextrose/saline combinations are hyperosmolar in the bag | Pulls water into the vascular space | Severe symptomatic hyponatremia or specific critical-care/neuro indications when ordered | Rapid sodium correction, fluid overload, pulmonary edema, vein irritation, extravasation injury |
See the full fluid and electrolyte balance guide for tonicity, sodium correction, and ABGs. Do not teach “D10W treats severe hyponatremia” — severe symptomatic hyponatremia is associated with carefully monitored hypertonic saline such as 3% NaCl, and dextrose-containing fluids require careful interpretation because dextrose is metabolized.
Access is not “central line only”
IV Complications You Must Recognize
| Complication | Key findings | First nursing thinking | Common actions |
|---|---|---|---|
| Infiltration | Cool skin, swelling, pallor/blanching, discomfort, slowed infusion | Non-vesicant fluid is leaking into tissue | Stop infusion, remove the peripheral IV per policy, elevate the extremity, apply warm/cold compress per policy, restart at a different site if needed |
| Extravasation | Burning/severe pain, swelling, tightness, blistering, tissue injury; vesicant/irritant medication | A vesicant or harmful medication/fluid is leaking into tissue | Stop infusion, disconnect tubing (do not flush), leave the catheter in place initially to aspirate residual drug, give antidote per policy, notify provider/pharmacy, elevate, then compress (cold for most vesicants; warm for vinca alkaloids/etoposide/oxaliplatin) |
| Phlebitis | Redness, warmth, tenderness, pain, palpable cord along the vein | Vein inflammation | Stop infusion, remove the IV, apply warm compress if appropriate, restart away from the affected vein, document with the facility scale, notify based on severity/policy |
| Local infection | Redness, warmth, purulent drainage, tenderness, possible fever | The catheter site may be infected | Remove the catheter per policy, culture if ordered, notify provider/RN, document, monitor for systemic infection |
| Fluid overload | Dyspnea, crackles, edema, JVD, hypertension or worsening oxygenation, sudden weight gain | Too much intravascular volume | Raise the head of the bed, slow/stop the infusion per policy/order, assess respiratory status, monitor oxygenation, notify provider/RN |
| Air embolism | Sudden dyspnea, chest pain, hypotension, cyanosis, tachycardia, altered mental status after line disconnection/air entry | Air has entered the circulation | Clamp/occlude the source, call rapid response, give high-flow oxygen, place in left lateral Trendelenburg if tolerated and not contraindicated, monitor ABCs |
| Occlusion | Pump alarm, no flow, resistance when flushing, possible swelling or pain | The line may be kinked, clotted, infiltrated, or malpositioned | Check tubing and site, do not force a flush, follow policy for troubleshooting/replacement |
Peripheral IV Site and Line Safety
A safe peripheral IV site is assessable, secure, and free from redness, warmth, swelling, drainage, pain, or leaking; infuses at the ordered rate; and is appropriate for the medication or fluid. Question use of an extremity with a dialysis fistula/graft, mastectomy/lymphedema-risk side (per policy), significant edema, infection, burns, trauma, impaired circulation, prior infiltration injury, or a stroke-affected limb when policy or condition makes it unsafe.
Site-care principles: perform hand hygiene before and after IV care, use aseptic technique, scrub access ports per policy, keep dressings clean/dry/intact, replace damp or soiled dressings, remove malfunctioning or symptomatic peripheral IVs promptly, and label tubing per policy. For aseptic technique and CLABSI prevention, see infection control.
How often to replace a peripheral IV
Central Lines, PICCs, and TPN
Central venous access devices include central lines, PICCs, tunneled catheters, implanted ports, and dialysis catheters. NCLEX may test strict aseptic technique, dressing integrity, CLABSI prevention, air embolism risk, line occlusion, catheter migration/dislodgement, TPN complications, bloodstream-infection cues, compatibility, and whether the access type fits the ordered therapy.
Central-line danger cues to report/escalate: fever/chills without another source, purulent drainage, redness/swelling/tenderness at the insertion site, new dyspnea or chest pain during line manipulation, a sudden catheter-length change, line disconnection, inability to flush, swelling of the neck/face/arm, and signs of sepsis.
TPN is high-risk because it is hypertonic and glucose-rich. Monitor for hyperglycemia, hypoglycemia if stopped abruptly, infection, fluid overload, electrolyte imbalance, line contamination, and compatibility problems. Do not use a TPN line casually for incompatible medications unless policy and orders allow.
Blood Product Administration and Reactions
Before blood administration, confirm per facility policy (commonly a two-nurse check): provider order, client identity, blood component and unit number, blood type and compatibility/crossmatch, consent, expiration time, baseline vital signs, appropriate venous access, filtered blood tubing, and normal saline as the only compatible fluid.
During the transfusion, start slowly per policy, stay with the client for the initial monitoring period (commonly the first 15 minutes), recheck vital signs per policy, and teach the client to report chills, itching, chest/back pain, dyspnea, anxiety, or feeling “not right.” A unit is commonly completed within 4 hours.
Suspected transfusion reaction — stop first
IV Medication Compatibility and High-Risk Infusions
Before giving IV medications, confirm compatibility with the fluid and other medications, whether dilution or a pump is required, vesicant/irritant status, whether central access is needed, whether cardiac monitoring is required, the patient’s allergies/renal function/labs, and whether the rate is safe. Review the pharmacology behind high-alert IV medications.
| Therapy | NCLEX concern |
|---|---|
| Potassium chloride | Never IV push; verify dilution, pump, rate, renal function, and cardiac monitoring when indicated |
| Vesicants | Extravasation risk; verify patency and correct access |
| Vancomycin / irritating antibiotics | Phlebitis/infiltration risk, rate reactions, compatibility |
| Heparin | Bleeding risk, pump/rate accuracy, lab monitoring |
| Insulin infusion | Glucose and potassium monitoring |
| TPN | Infection, hyperglycemia, compatibility, central access/policy |
| Blood products | Verification, first-15-minute monitoring, reaction response |
IV Flow Rate Calculations
mL/hr = total volume ÷ time in hours. Example: 1000 mL over 8 hours = 1000 ÷ 8 = 125 mL/hr.
gtt/min = volume × drop factor ÷ time in minutes. Example: 1000 mL over 8 hours with 15 gtt/mL tubing → 8 × 60 = 480 minutes; 1000 × 15 ÷ 480 = 31.25 → 31 gtt/min.
Calculation safety check: Does the rate make clinical sense? Did I convert hours to minutes and use the correct drop factor? Did I round correctly? Is the patient at risk for fluid overload? Does this require a pump, or should the order be clarified?
How NGN Tests IV Therapy
IV therapy suits NGN case studies because complications evolve over time across tabs such as the MAR, IV orders, vital signs, intake/output, nursing notes, labs, IV-site assessment, and blood-bank information. Work the NGN method and watch for these item formats:
| NGN item type | IV therapy example |
|---|---|
| Case study | Track IV site swelling, pain, infusion rate, and medication risk over time |
| Matrix | Mark findings as expected, concerning, or requiring immediate follow-up |
| Bow-tie | Identify the complication, priority actions, and monitoring parameters |
| SATA | Select actions for extravasation, transfusion reaction, or fluid overload |
| Highlight | Identify cues showing infiltration, phlebitis, or a transfusion reaction |
| Calculation | Determine mL/hr or gtt/min and verify reasonableness |
Practice IV Therapy Questions
Practice IV therapy questions with fluids, complications, calculations, blood products, and NGN-style rationales that explain why unsafe distractors are wrong.
Start PracticingNCLEX-Style Practice Questions
Question 1 — Infiltration
A client receiving 0.9% sodium chloride through a peripheral IV reports discomfort. The site is cool, pale, and swollen, and the infusion is slowing.
What is the best interpretation and action?
- A. Phlebitis — apply a warm compress and continue the infusion
- B. Infiltration — stop the infusion and remove the peripheral IV per policy
- C. Infection — culture the site and continue the infusion
- D. Air embolism — place the client in Trendelenburg
Rationale: Coolness, pallor, swelling, discomfort, and slowed flow suggest infiltration of a non-vesicant fluid. Stop the infusion, remove the peripheral catheter per policy, elevate the extremity, apply compresses per policy, and restart at another site if IV therapy must continue.
Question 2 — Extravasation
A client receiving a vesicant IV medication reports burning pain at the site. The area is swollen and tight.
What should the nurse do first?
- A. Remove the IV immediately and discard the catheter
- B. Stop the infusion and leave the catheter in place initially
- C. Flush the line with normal saline
- D. Apply pressure to disperse the medication
Rationale: Suspected vesicant extravasation requires stopping the infusion immediately. The catheter is left in place initially to aspirate residual drug and give an antidote per policy — the opposite of the routine infiltration rule. Do not flush or apply pressure, which would spread the vesicant.
Question 3 — Fluid overload (SATA)
A client receiving IV fluids develops dyspnea, crackles, oxygen saturation of 89%, and new jugular venous distention.
Which actions are appropriate? (Select all that apply.)
- A. Raise the head of the bed
- B. Slow or stop the infusion according to policy/order
- C. Assess respiratory status and oxygen saturation
- D. Encourage the client to drink more fluids
- E. Notify the provider/RN according to urgency and role
- F. Document only and reassess at the next scheduled vital-sign check
Rationale: The findings suggest fluid overload with impaired oxygenation. Support breathing, reduce the source of excess fluid, assess respiratory status, and escalate. Oral fluids and delayed reassessment are unsafe.
Question 4 — Blood transfusion reaction
A client receiving packed red blood cells develops chills, back pain, fever, and anxiety 10 minutes after the transfusion starts.
What is the priority action?
- A. Slow the transfusion rate
- B. Stop the transfusion immediately
- C. Administer acetaminophen and continue
- D. Document the finding after the transfusion is complete
Rationale: Chills, back pain, fever, and anxiety may indicate a transfusion reaction. Stop the transfusion immediately, keep the line open with normal saline using new tubing, assess the client, notify the provider and blood bank, and follow the reaction protocol.
Question 5 — Flow rate
The provider prescribes 1000 mL of lactated Ringer's solution to infuse over 10 hours.
What pump rate should the nurse set?
- A. 50 mL/hr
- B. 75 mL/hr
- C. 100 mL/hr
- D. 125 mL/hr
Rationale: 1000 mL ÷ 10 hr = 100 mL/hr.
Common IV Therapy Traps
Trap 1: Removing the catheter during extravasation
For a non-vesicant infiltration, removing a peripheral IV is usually appropriate. For vesicant extravasation, the catheter is left in place initially to aspirate residual drug or give an antidote per policy.
Trap 2: Treating all swelling as infiltration
Cool/pale swelling suggests infiltration; redness/warmth/pain with a palpable cord suggests phlebitis; severe pain/blistering with a vesicant suggests extravasation.
Trap 3: “Central line only” as a universal rule
Some high-osmolality, vesicant, or long-duration therapies need central access, but the answer depends on the specific fluid, medication, concentration, order, policy, and patient risk.
Trap 4: Forgetting the patient during pump alarms
Do not stare only at the pump. Assess the patient, the IV site, the tubing, the order, and the infusion.
Trap 5: Continuing blood during a suspected reaction
Stop the transfusion first when a reaction is suspected. Do not simply slow it and continue.
Trap 6: Forcing a flush
Never force a flush against resistance. Resistance may indicate occlusion, malposition, infiltration, or another problem.
Trap 7: Documenting before acting
Document after urgent safety actions are started — not first — when the client has respiratory distress, a suspected reaction, extravasation, or air-embolism symptoms.
Practice IV Therapy With RN Test Pro
IV therapy improves when you practice pattern recognition:
- Match fluid type to patient condition
- Distinguish infiltration, extravasation, and phlebitis
- Calculate rates accurately
- Recognize fluid overload and transfusion reactions
- Choose safe first actions
- Evaluate the patient’s response
RN Test Pro helps you practice IV fluids, complications, calculations, blood products, central lines, TPN, and NGN-style scenarios with rationales that explain why unsafe distractors are wrong. Turn your review into a schedule with an NCLEX study plan.
Frequently Asked Questions
What IV topics are most important for NCLEX?
High-yield topics include IV fluid types, infiltration, extravasation, phlebitis, fluid overload, air embolism, IV calculations, compatibility, blood transfusion reactions, central-line safety, and TPN complications.
What is the difference between infiltration and extravasation?
Infiltration is leakage of a non-vesicant fluid into surrounding tissue. Extravasation is leakage of a vesicant or harmful medication/fluid into tissue and can cause severe injury.
What should the nurse do first for infiltration?
Stop the infusion and remove the peripheral IV per policy, then elevate the extremity, apply compresses as directed, assess severity, document, and restart IV access at a different site if needed.
What should the nurse do first for extravasation?
Stop the infusion. Leave the catheter in place initially for possible aspiration or antidote administration, notify provider/pharmacy per policy, and do not flush the line.
What should the nurse do for a suspected air embolism?
Clamp or occlude the source, call rapid response, give high-flow oxygen, position left lateral Trendelenburg if tolerated and not contraindicated, and monitor airway, breathing, circulation, and neurologic status. Stopping the air and getting help come before positioning.
What IV fluid is usually used with blood products?
Only 0.9% normal saline is compatible with blood products (not lactated Ringer's or dextrose solutions). Use filtered blood tubing and follow facility policy and blood-bank procedure.
How long should blood hang?
Follow facility policy, but a blood product unit is commonly completed within 4 hours of initiation to reduce bacterial-growth risk.
What is the fastest way to calculate mL/hr?
Divide total volume by total hours. Example: 1000 mL over 8 hours equals 125 mL/hr.
What is the biggest NCLEX trap in IV therapy?
Choosing an action that sounds active but does not stop the source of harm. If the infusion or line is causing the problem, protect the patient first.
Build IV Therapy Confidence the Way NCLEX Tests It
Practice IV fluids, complications, calculations, blood products, and central-line scenarios with clinical-judgment rationales, and track your weak areas.
Get Started FreeRelated Topics
Fluid & Electrolytes
Tonicity, sodium correction, fluid overload, and ABGs.
Pharmacology Review
High-alert IV medications, compatibility, and adverse effects.
Reduction of Risk Potential
Complication monitoring and site assessment.
Physiological Adaptation
When IV complications progress to shock or respiratory distress.
Infection Control
Aseptic technique, CLABSI prevention, and dressing care.
NCLEX Question Types
SATA, matrix, bow-tie, highlight, and calculation items.