Mental Health for NCLEX-PN: Psychosocial Integrity, Safety, and Therapeutic Communication
Mental health questions on the NCLEX-PN test whether you can recognize psychosocial cues, communicate therapeutically, protect client safety, and report important changes within practical/vocational nursing scope.
This topic is not just about memorizing psychiatric diagnoses. The exam wants to know whether you can answer questions such as:
- What statement shows suicide risk?
- Which response is therapeutic?
- What should the PN do first during a panic attack?
- How should the PN respond to hallucinations or delusions?
- What behavior requires immediate reporting?
- Which action is safe within PN scope?
The safest approach is to focus on safety, communication, scope, and escalation.
PN Mental Health at a Glance
On the NCLEX-PN, mental health content appears mainly in Psychosocial Integrity, which accounts for 9–15% of NCLEX-PN content-area items (see the full Client Needs blueprint). Psychosocial Integrity includes:
- Therapeutic communication and emotional support
- Coping and stress management
- Grief, loss, and end-of-life support
- Behavioral health conditions
- Substance misuse, withdrawal, and overdose cues
- Crisis intervention
- Sensory and perceptual alterations
- Violence risk to self or others
- Trauma-informed care and therapeutic environment
Scope reminder
About this guide
What Mental Health Questions Test on the NCLEX-PN
Mental health questions often test judgment more than vocabulary. A strong PN answer usually does one of these:
- Keeps the client safe
- Uses therapeutic communication
- Avoids judgment, advice, false reassurance, and arguing
- Recognizes suicide, self-harm, violence, or abuse cues
- Reports new, worsening, or unsafe behavior
- Follows the plan of care and facility policy
- Documents exact statements and objective behavior
- Provides direct care within scope
A weak answer often does one of these:
- Tells the client what to do
- Says “everything will be fine”
- Asks “why” in a blaming way
- Argues with hallucinations or delusions
- Threatens restraints or punishment
- Leaves a suicidal client alone
- Documents before addressing immediate safety
- Acts outside PN scope or without an order/protocol
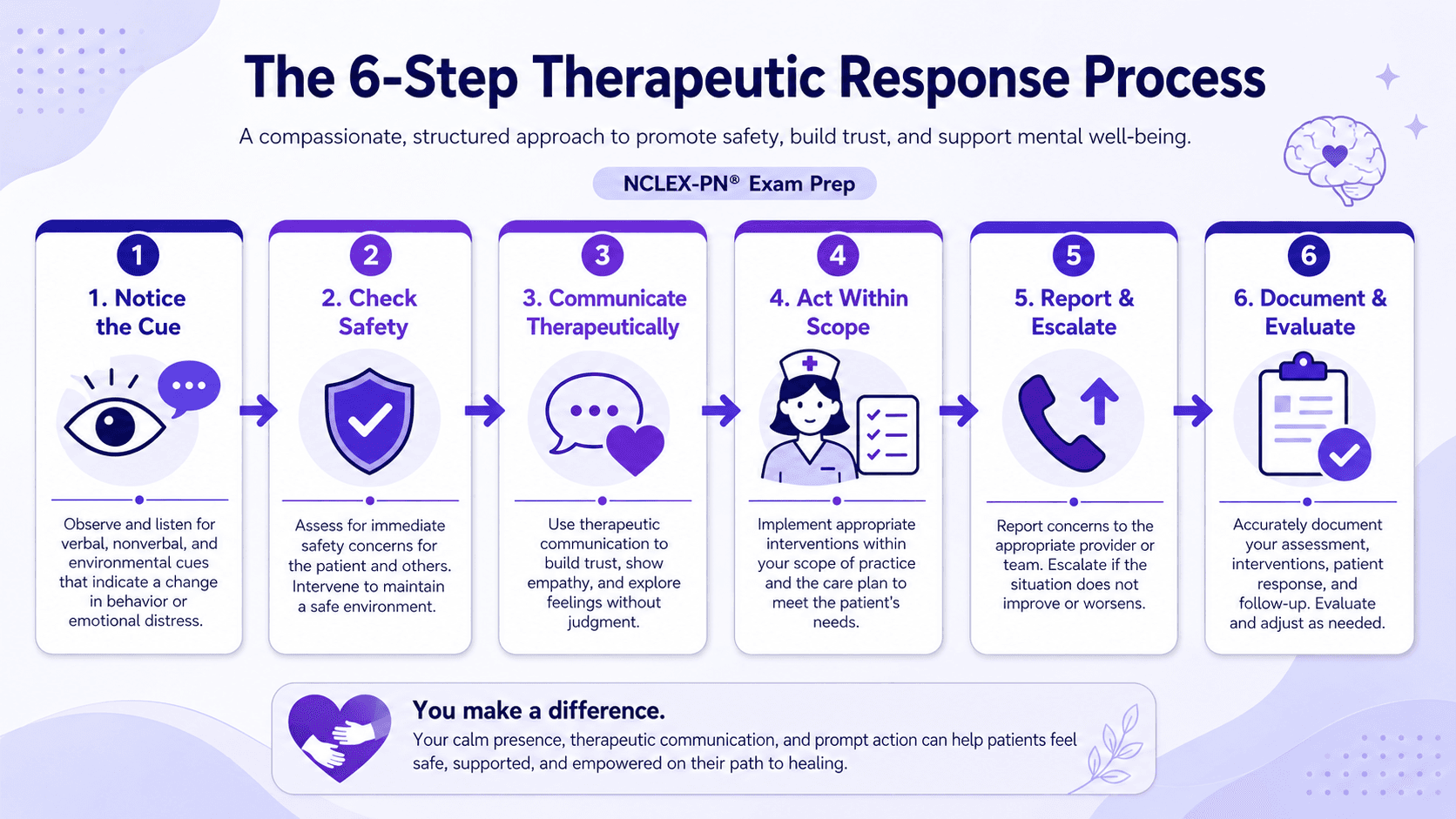
The PN Mental Health Decision Framework
Use this six-step method for mental health questions. It mirrors the same clinical judgment the exam measures.
1. Notice the cue
Ask: What did the client say or do that matters? Important cues include statements like “I want to die,” “my family would be better off without me,” or “the voices are telling me to hurt myself”; new agitation, pacing, clenched fists, or threats; refusal to eat because of a delusion; sudden confusion or withdrawal; panic with inability to focus; tremors, sweating, hallucinations, or seizures during withdrawal; and signs of abuse, neglect, or a trauma response.
2. Check immediate safety
Ask: Is there a risk of harm to self or others? Safety comes before routine teaching, documentation, or long conversation. If a safety risk is present, the PN should stay with the client or maintain observation according to policy, remove obvious hazards if safe and allowed, call for help, and notify the RN or provider immediately.
3. Use therapeutic communication
The first response should usually acknowledge the client’s feeling and invite more information — for example, “That sounds frightening. Tell me more about what you are hearing,” or “When you say you cannot go on, are you thinking about killing yourself?”
4. Act within PN scope
PN-level actions may include staying with the client, using a calm low voice, reducing stimulation, encouraging slow breathing during panic, offering simple choices, reinforcing coping strategies already in the plan of care, monitoring for medication effects, obtaining focused data, and supporting nutrition, hydration, hygiene, rest, and safety. Avoid actions that require independent diagnosis, new medication changes, independent treatment planning, or physical restriction without legal/policy authority.
5. Report or escalate
Report immediately when the client has suicidal thoughts/plan/means/intent, homicidal thoughts or threats, command hallucinations, escalating agitation or violence risk, severe withdrawal symptoms, new confusion or sudden behavior change, refusal of essential care with safety risk, possible abuse or exploitation, or potentially serious medication side effects.
6. Document objectively
Document after immediate safety actions are started, using exact client statements when important — for example, “Client stated, ‘I want to end it tonight.’” or “Client refused meal, stating, ‘The food is poisoned.’” Avoid judgmental wording such as “crazy,” “attention-seeking,” or “manipulative.”
Therapeutic vs Non-Therapeutic Communication
The NCLEX-PN frequently asks you to pick the most therapeutic response. These tables show high-yield examples.
| Communication type | Therapeutic example | Why it works |
|---|---|---|
| Open-ended question | “Tell me more about what has been happening.” | Encourages expression without forcing a yes/no answer. |
| Reflection | “You sound overwhelmed.” | Shows the nurse is listening and helps the client explore feelings. |
| Clarification | “What do you mean when you say you are ‘done’?” | Clarifies ambiguous or unsafe statements. |
| Restating | “You are saying the voices become worse at night.” | Confirms understanding. |
| Silence | Sitting quietly with the client. | Gives time to think and speak. |
| Validation | “It makes sense that you feel scared right now.” | Acknowledges emotion without agreeing with unsafe beliefs. |
| Non-therapeutic response | Why it is wrong | Better approach |
|---|---|---|
| “You should just calm down.” | Gives advice and may feel dismissive. | “I can see you are upset. I will stay with you.” |
| “Everything will be fine.” | False reassurance. | “This feels scary. Let’s focus on what is happening right now.” |
| “Why would you say that?” | Can sound blaming or accusatory. | “What happened before you started feeling this way?” |
| “The voices are not real.” | Argues with the client’s perception. | “I do not hear the voices, but I can see they are frightening to you.” |
| “If you do not stop, we will restrain you.” | Threatening and unsafe. | “I want to help keep everyone safe. Let’s move to a quieter area.” |
| “My cousin had the same problem.” | Shifts focus to the nurse. | “Tell me how this has been affecting you.” |
Suicide, Self-Harm, and Violence Risk: Safety First
Any statement about wanting to die, self-harm, hopelessness, being a burden, or not wanting to live must be taken seriously. If a client makes a suicidal statement, the PN should:
- Stay with the client or maintain observation according to facility policy.
- Ask direct safety questions when appropriate: “Are you thinking about killing yourself? Do you have a plan? Do you have access to the means? Do you intend to act on this?”
- Remove obvious hazards if safe, allowed, and policy-directed.
- Notify the RN and provider immediately.
- Follow suicide precautions per facility protocol.
- Document exact statements and actions taken.
Do not choose these answers
Common Mental Health Presentations
| Presentation | Cues to recognize | PN actions that fit NCLEX-PN |
|---|---|---|
| Depression | Persistent sadness, hopelessness, anhedonia, sleep/appetite change, low energy, suicidal thoughts | Use therapeutic communication, ask direct safety questions if indicated, support routine and self-care, report suicidal statements or worsening symptoms. |
| Anxiety or panic | Fear, restlessness, trembling, shortness of breath, palpitations, feeling of doom | Stay with the client, use a calm voice, reduce stimulation, guide simple breathing/grounding if the client can follow, report escalation or medical concerns. |
| Psychosis | Hallucinations, delusions, paranoia, disorganized speech, impaired reality testing | Do not argue; acknowledge the feeling; focus on safety; reduce stimulation; report command hallucinations or danger cues. |
| Mania | Decreased need for sleep, pressured speech, impulsivity, grandiosity, poor judgment, agitation | Reduce stimulation, set simple limits, offer easy-to-consume food/fluids, monitor for exhaustion and safety, report escalation. |
| Substance withdrawal | Tremors, sweating, agitation, hallucinations, nausea/vomiting, seizures, unstable vitals | Monitor closely, maintain safety, report promptly, follow the withdrawal protocol and ordered medications. |
| Cognitive impairment or delirium | Confusion, disorientation, agitation, change from baseline, unsafe behavior | Reorient calmly, maintain safety, reduce hazards, collect focused data, report sudden changes. |
| Grief or loss | Sadness, crying, anger, guilt, changes in sleep or appetite after a loss | Listen, support expression, avoid clichés, report suicidal ideation, inability to function, or severe/worsening symptoms. |
| Trauma response | Withdrawal, panic, dissociation, hypervigilance, refusal to continue assessment | Pause when safe, respect boundaries, use calm reassurance, offer choice, avoid unwanted touch, report distress or safety concerns. |
Assessment Tools: Know the Purpose, Not Just the Score
NCLEX-PN questions may mention mental health screening tools. The most important point is usually what the tool screens for and what the nurse should report — not memorized cutoffs. In real NCLEX-style items, scoring guidance should be provided when interpretation is required.
| Tool | What it screens for | PN exam takeaway |
|---|---|---|
| PHQ-9 | Depression symptoms and a self-harm item | Report concerning scores, suicidal thoughts, or worsening symptoms; do not diagnose. |
| GAD-7 | Anxiety symptoms | Recognize anxiety severity cues and report moderate/severe or worsening symptoms. |
| C-SSRS | Suicide ideation and behavior | Focus on suicidal thoughts, plan, intent, means, behavior, safety, and escalation. |
| MMSE or similar cognitive screen | Cognitive impairment | Report abnormal findings or sudden change from baseline; distinguish screening from diagnosis. |
Trauma-Informed and De-Escalation Principles
Trauma-informed care means the nurse avoids actions that may increase fear, shame, or loss of control. Use a calm voice, respectful distance, simple choices, permission before touch, clear explanation before procedures, privacy when possible, a low-stimulation environment, boundaries without threats, and collaboration with the care team. If the client becomes more distressed, stop nonurgent questioning, maintain safety, and notify the RN or appropriate clinician.
How NGN Tests PN Mental Health
Mental health content can appear in traditional and NGN-style questions. For format strategy, see the PN NGN strategies guide, the broader Next Generation NCLEX overview, and the full list of NCLEX question types.
| Item type | How mental health may appear |
|---|---|
| Multiple choice | Choose the most therapeutic response or the first safety action. |
| SATA | Select appropriate actions for suicide precautions or panic management. |
| Matrix | Mark each finding as expected, concerning, or requiring follow-up. |
| Highlight | Identify statements that suggest suicide risk, violence risk, withdrawal, or psychosis. |
| Bow-tie | Connect the priority concern with nursing actions and monitoring. |
| Case study | Track behavior, medication effects, safety risk, and communication across tabs. |
For every format, ask: What cue matters? Is safety threatened? What response is therapeutic? What is within PN scope? What must be reported now? What should be documented?
PN-Level Practice Scenarios
Scenario 1 — Suicidal statement
A client says, “I feel like life is not worth living anymore. My family would be better off without me.”
What is the best PN action?
- A. Tell the client the family would be very upset if anything happened
- B. Stay with the client and ask directly about suicidal thoughts, plan, means, and intent
- C. Document the statement and check on the client later
- D. Change the subject to a more positive topic
Rationale: The client’s statement may indicate suicide risk. The PN should stay with the client, ask direct safety questions, notify the RN/provider immediately, and follow suicide precautions per policy. False reassurance, changing the subject, and delayed follow-up are unsafe.
Scenario 2 — Paranoid delusion about food
A client with schizophrenia says, “The food is poisoned.” The client appears frightened and refuses to eat.
What is the best response?
- A. “That is not true. The food is safe.”
- B. “I can see this is frightening. Would you like a sealed food item instead?”
- C. “You need to eat or you will get weaker.”
- D. “Your medication will make those thoughts go away.”
Rationale: Do not argue with a delusion. Acknowledge the feeling, maintain safety, and offer a practical option that supports nutrition without reinforcing the delusion. Report refusal to eat or worsening paranoia.
Scenario 3 — Escalating agitation
A client is pacing, clenching fists, and raising their voice. The client says, “Leave me alone!”
What is the best PN response?
- A. “You need to calm down right now.”
- B. “If you do not stop, restraints will be used.”
- C. “I can see you are upset. I will give you space, but I am staying nearby to keep everyone safe.”
- D. “Let’s go outside for a walk.”
Rationale: The PN should use calm, nonthreatening communication, maintain safety, allow space, and seek help if needed. Threats and commands can escalate agitation. Leaving the unit or going outside may be unsafe depending on policy and client status.
Scenario 4 — Mania and a request to leave
A client in a manic episode says they are leaving the unit to “start a business today.” The client is not on a legal hold.
What is the PN’s priority action?
- A. Physically prevent the client from leaving
- B. Tell the client they are not thinking clearly and cannot leave
- C. Notify the RN/provider and follow facility policy for safety, elopement, or leaving against medical advice
- D. Ignore the statement because the client is not on a legal hold
Rationale: The PN should escalate immediately and follow facility policy. If the client is not legally detained, the PN should not physically prevent leaving unless legally authorized and policy-directed. The PN should maintain safety and document objective behavior.
Scenario 5 — Trauma response during assessment
During a routine assessment, a client with a trauma history becomes quiet, stares ahead, and says, “I do not want to talk about this.”
What is the best PN action?
- A. Continue because the assessment must be completed
- B. Stop the nonurgent questioning, speak calmly, and offer a break
- C. Hold the client’s hand to ground them
- D. Ask, “Why are you acting like this?”
Rationale: Trauma-informed care prioritizes safety, trust, choice, and control. Stop nonurgent questioning when safe, offer space, avoid unwanted touch, and notify the RN if distress continues or safety concerns appear.
Practice PN Psychosocial Integrity Questions
Practice PN Psychosocial Integrity questions with safety-focused rationales that explain why unsafe or out-of-scope distractors are wrong.
Start PracticingCommon NCLEX-PN Mental Health Traps
Trap 1: False reassurance
Avoid “Everything will be fine.” Choose “This feels frightening. Tell me what is happening.”
Trap 2: Arguing with delusions
Avoid “That is not real.” Choose “I do not hear the voices, but I can see they are upsetting you.”
Trap 3: Asking “why”
Avoid “Why would you do that?” Choose “What happened before you started feeling this way?”
Trap 4: Documenting first
Documentation matters, but safety comes first when the client is suicidal, violent, severely agitated, or medically unstable.
Trap 5: Threatening restraints
Restraints and seclusion are not punishment and should not be threatened. Follow facility policy and use the least restrictive safe intervention.
Trap 6: Acting outside PN scope
Do not choose independent diagnosis, new treatment planning, medication changes without an order/protocol, or legal detention decisions.
Trap 7: Ignoring substance withdrawal
Withdrawal can become medically dangerous. Report severe agitation, hallucinations, seizures, unstable vital signs, or worsening confusion.
Practice PN Psychosocial Integrity With RN Test Pro
Mental health questions improve when you practice the reasoning pattern:
- Recognize safety cues
- Choose therapeutic communication
- Stay within PN scope
- Report significant changes
- Document objectively
- Evaluate whether the client is safer or more stable
RN Test Pro helps you practice PN-level Psychosocial Integrity questions, NGN-style scenarios, therapeutic communication, crisis response, and rationales that explain why unsafe or out-of-scope distractors are wrong. Turn it into a schedule with an NCLEX study plan, and review how scoring and partial credit work for SATA and matrix items.
Frequently Asked Questions
What percentage of the NCLEX-PN is Psychosocial Integrity?
Psychosocial Integrity accounts for 9–15% of NCLEX-PN content-area items.
What is the most important rule for mental health NCLEX questions?
Safety comes first. Any suicide, self-harm, violence, abuse, severe agitation, withdrawal, or command-hallucination cue requires immediate attention and escalation.
Should I ask a client directly about suicide?
Yes, when the client makes a concerning statement or shows warning signs. Direct questions about suicidal thoughts, plan, means, and intent are appropriate and safer than avoiding the topic.
What communication responses are usually therapeutic?
Open-ended questions, reflection, clarification, restating, silence, validation, and calm presence are usually therapeutic when used appropriately.
What responses are usually non-therapeutic?
Giving advice, false reassurance, judging, changing the subject, arguing, asking blaming “why” questions, and making threats are usually non-therapeutic.
What should the PN do for hallucinations or delusions?
Do not argue or reinforce the belief. Acknowledge the client’s feeling, focus on safety, reduce stimulation, monitor behavior, and report danger cues or worsening symptoms.
Do I need to memorize every mental health scale score?
No. Know what common tools screen for and what findings require reporting. If an NCLEX-style item requires score interpretation, the scoring information should be provided or clearly inferable.
What is the PN role during a psychiatric crisis?
Maintain safety, use calm therapeutic communication, collect focused data, follow facility policy, notify the RN/provider, and document objective findings and exact statements.
Build PN Mental Health Confidence the Way NCLEX Tests It
Practice PN Psychosocial Integrity and mental health scenarios with safety-focused, scope-safe rationales, and track your weak areas.
Get Started FreeRelated Topics
Psychosocial Integrity
Where mental health sits in the Client Needs blueprint.
PN NGN Strategies
A scope-safe method for PN clinical judgment items.
Clinical Judgment (CJMM)
The six-step model behind NGN reasoning.
NCLEX Question Types
Highlight, matrix, SATA, bow-tie, and more.
RN vs PN NCLEX
How scope and emphasis differ between the exams.
NCLEX-PN Overview
The PN hub: scope, blueprint, and exam-day prep.